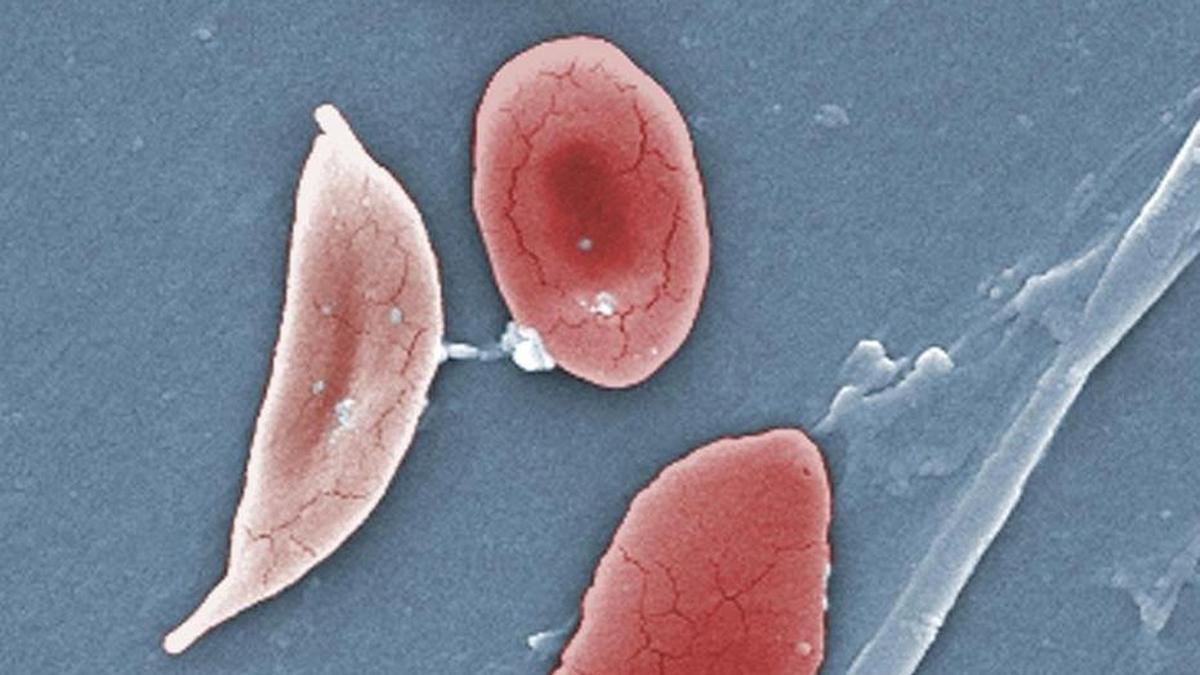
In India, the gap between a mother and safe care is often measured in hours: a delayed referral, a missed antenatal visit, a danger sign that no one caught in time.
The country has cut maternal and newborn deaths sharply over the past decade; yet the burden that remains is among the largest in the world.
It is in exactly that gap, between an early warning and a late response, that Artificial Intelligence (AI) is now being asked to help.
Its most useful contribution will likely be far more ordinary than the futuristic promises suggest: noticing trouble a little earlier, while there is still time to act.
The country’s gains are worth stating plainly.
Government data records a fall in the maternal mortality ratio from 130 deaths per lakh live births in 2014-16 to 93 in 2019-21, and then to 88 in 2021-23.
Neonatal mortality declined from 26 per 1,000 live births in 2014 to 19 in 2021.
These gains, however, sit within a larger and still daunting picture.
Globally, the World Health Organization (WHO) estimates that about 2,60,000 women died during pregnancy, childbirth or the weeks that followed in 2023, and UNICEF places newborn deaths in the first month of life at 2.3 million in 2024, roughly 6,200 a day.
Each figure represents a warning some health system failed to register, a mother it could not reach, or a complication it recognised too late.
The many challenges of ensuring maternal and child health in India Why prediction This is where prediction can help.
Much of the raw material already exists within the system: antenatal records, laboratory results, blood pressure trends, maternal age, anaemia status, obstetric history, birth weight, gestational age, facility data and social risk indicators.
A model that reads across these can flag a pregnancy that needs closer observation, identify a woman quietly slipping out of follow-ups, or point to early signals of preterm birth, pre-eclampsia, neonatal sepsis or respiratory distress before they become emergencies.
None of this saves lives on its own.
Doctors, nurses, midwives, ASHA workers and the public health teams behind them save lives.
What a model offers is a clearer sense of who needs attention first.
A prediction matters only when it reaches the right person at the right moment and is tied to a concrete response: an additional visit, a referral, a test, transport to a facility, emergency care.
A warning that reaches no one changes nothing.
AI can assist in detecting foetal abnormalities, however, clinical decisions require medical expertise How it can work One Indian programme already shows what this can look like.
ARMMAN, a Mumbai-based non-profit, runs mMitra, a free service that has delivered preventive-care voice messages to expectant and new mothers since 2013.
Many women, often those most at risk, drift away from the calls within weeks.
Working with researchers at Google and IIT Madras, ARMMAN built a model that predicts who is likely to disengage, so its limited team of health workers can reach those mothers first.
In testing, drop-offs among high-risk women fell by close to a third.
The lesson is not that the algorithm was clever; it is that a useful prediction was placed in the hands of people who could act on it.
Successes like that remain the exception.
Much healthcare AI fails at exactly this point.
The difficult task is not building one more model; it is building dependable decision support around it, and most pilots never make that transition.
They are trained on clean datasets and then confront the real world, where data is incomplete, delayed and scattered across systems that do not communicate.
Built on a weak foundation, even a sophisticated algorithm returns weak and sometimes biased results, presented with misleading confidence.
Preventing stillbirths requires redefining parameters, upgrading maternal care and generating better data Where the thrust needs to be The unglamorous work therefore carries the weight: trustworthy data pipelines, genuine interoperability, privacy safeguards, clinical validation and monitoring that continues well beyond launch.
Continuity of care belongs on that list.
Recent figures from the National Family Health Survey - 6 show the proportion of mothers receiving at least four antenatal visits rising from 58.5% to 65.2%.
That is an improvement, but it still leaves many pregnancies without the recommended follow-ups.
A model can indicate who is being missed; it cannot create the staff, transport or clinic hours required to reach them.
There is also a temptation to overstate what AI can do, and it deserves resistance.
Outcomes for mothers and newborns are shaped by far more than clinical risk.
They turn on nutrition, the distance to a facility, household income, the means to travel, education, family support and the condition of local health infrastructure.
An algorithm blind to these factors can report impressive accuracy while overlooking the women in greatest danger.
Such systems must therefore be explainable, audited for bias and kept under human supervision.
A clinician should be able to ask why a patient has been flagged as high risk and receive an answer.
A black box does not meet that standard.
Better-informed AI systems are needed for better health messaging Data-care collaborations The honest framing is one of partnership between data science and frontline care.
Used well, it shifts a health system from recording what has already happened towards preventing what might.
It locates risk earlier, directs outreach more precisely and channels limited resources towards the mothers and newborns who need them most.
None of this happens automatically.
It requires governance, a measure of humility and clear accountability when the model is wrong.
Algorithms by themselves will not save a single newborn.
Built on sound data, designed responsibly and embedded in care that can actually respond, they can help the people who do. (Karan Tejpal is an AI and analytics professional with expertise in healthcare analytics, public health data systems and predictive analytics.